

Once viewed primarily as a fertility disorder, PCOS is being reframed as a systemic endocrine and metabolic disease, opening the door to earlier diagnosis, more accurate risk profiling, and more personalized care.
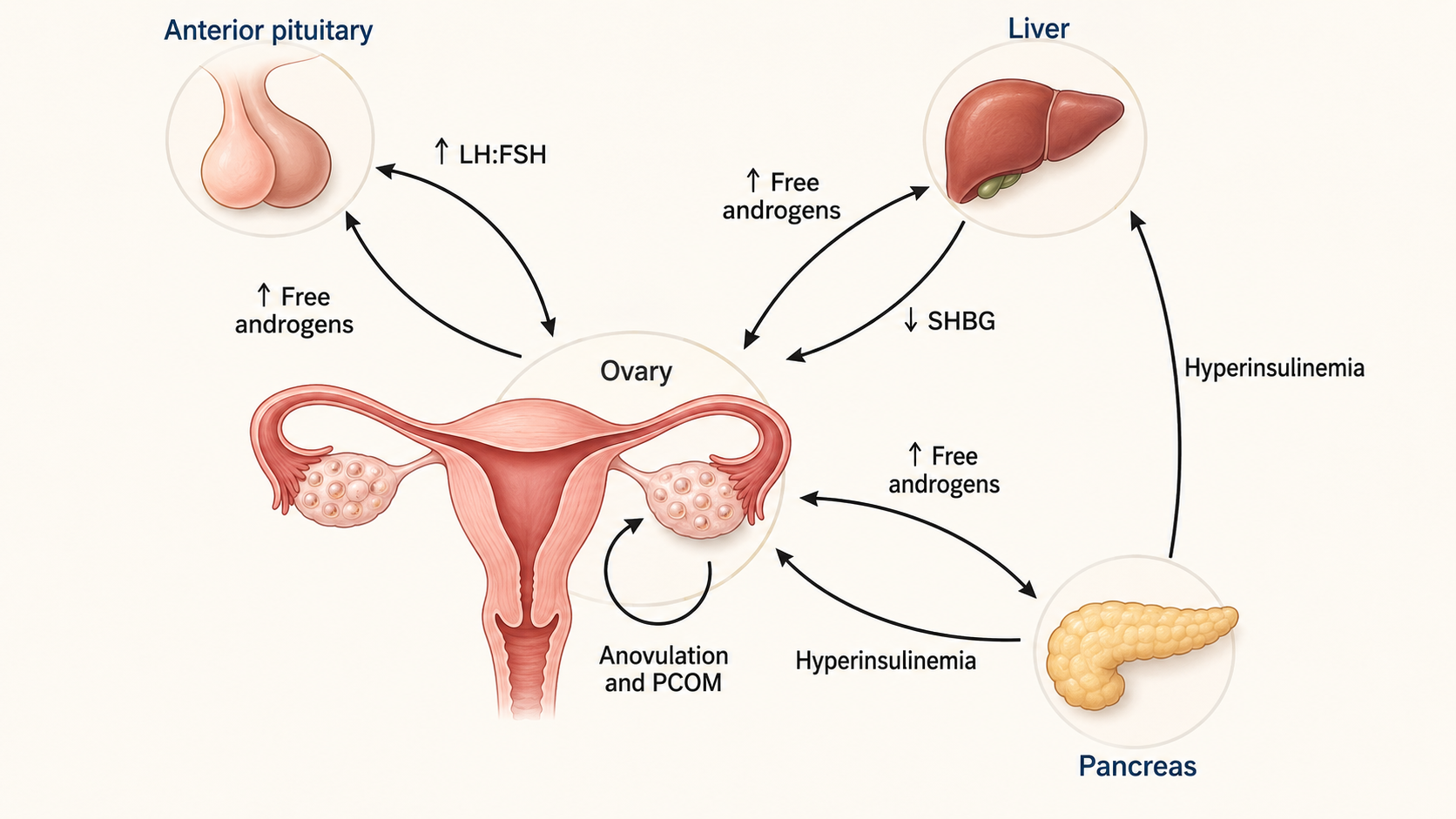
Pathophysiology of PCOS/PMOS. PCOS/PMOS is a complex syndrome involving multiple feedback loops in the anterior pituitary gland, liver, pancreas, and ovaries, ultimately leading to a hyperandrogenic state. In the pituitary gland, LH is released in greater amounts than FSH and stimulates the membranous cells of the ovary to increase androgen production. Androgens then stimulate the pituitary gland to release LH and FSH. Increased androgens also act on the liver, decreasing SHBG and increasing circulating free androgens. Finally, at the level of the pancreas, androgens cause hyperinsulinemia, resulting in a decrease in SHBG. Insulin also acts on theca cells to promote androgen release. All of these factors cause HA, leading to anovulation and PCOM in the ovary. LH, luteinizing hormone; FSH, follicle-stimulating hormone. SHBG, sex hormone binding globulin; AI-assisted redrawing based on Figure 1 from Chan JL, Masini I, Pisarska MD, “Polyendocrine metabolic ovarian syndrome (PMOS)/polycystic ovary syndrome (PCOS): current and future trends”, Journal of Clinical Investigation, 2026;136(12). https://www.jci.org/articles/view/202824. The original article is published under the Creative Commons Attribution 4.0 International License.
In a recently published comprehensive review, clinical research journalresearchers synthesized decades of research on polycystic ovary syndrome (PCOS) to elucidate the changing diagnostic paradigm surrounding the disease. We review the interactions between genetic, epigenetic, environmental, metabolic, and neuroendocrine factors that can contribute to disease development, phenotypic variation, and long-term complications, as well as novel targeted approaches to improve patient outcomes.
The results of this review highlight that the management of PCOS, recently proposed to be renamed polyendocrine-metabolic ovarian syndrome (PMOS), has long been hampered by diagnostic inconsistencies and symptom-focused treatments. The paper concludes by suggesting that PMOS treatment is moving from its “one-size-fits-all” roots to personalized, multisystem medicine that can support more targeted future treatments for this highly prevalent but poorly understood endocrine disease.
background
Decades of research and clinical reports have identified polycystic ovary syndrome (PCOS) as the most common endocrine disease among women of reproductive age worldwide. Research currently estimates that the condition affects between 5% and 20% of the world’s female population, depending on the diagnostic criteria used.
Unfortunately, despite the widespread prevalence of this disease, the exact biological mechanisms that cause this condition remain incompletely understood. As a result, researchers believe that current prevalence estimates may underestimate the true prevalence, potentially resulting in millions of patients being misdiagnosed or receiving inappropriate treatment.
Culturally and historically, PCOS has been viewed primarily as a fertility problem, as it is associated with irregular menstrual cycles and polycystic ovarian forms. However, the latest clinical insights reveal a much more systemic reality. Recent studies have demonstrated that this disorder is underpinned by hormonal and metabolic disorders, often involving elevated androgens and insulin resistance.
Scientists now know that this combination of reproductive, endocrine, and metabolic functions is associated with a patient’s lifetime risk of metabolic complications such as insulin resistance, type 2 diabetes mellitus (T2DM), and cardiovascular disease (CVD), but a definitive causal link between PCOS itself and CVD has not been established. New research has further linked this condition to clinically significant mental health issues such as depression and anxiety.
To better reflect the nature of this multisystem metabolism, an international consortium recently proposed renaming this condition polyendocrine metabolic ovary syndrome (PMOS).
About reviews
This comprehensive review aims to elucidate the complex structure of PMOS by synthesizing findings from clinical studies, genetic analyses, mechanistic studies, animal models, and novel in vitro platforms.
In particular, it assessed the implementation of the latest 2023 international evidence-based guidelines recommending the Rotterdam Criteria for adults. These criteria require individuals to meet two of three key diagnostic features: ovulatory dysfunction (OD), biochemical or clinical hyperandrogenism (HA), and polycystic ovarian morphology (PCOM), excluding other hormonal disorders.
Within the realm of diagnostic data, this review details advanced biochemical tracking, including measurement of total testosterone using liquid chromatography tandem mass spectrometry (LC-MS/MS) and mapping of antral follicle number using pelvic transvaginal ultrasound with a broadband transducer (>8 MHz). Additionally, while this paper evaluates its validity as an objective, non-invasive alternative (“surrogate”) for ultrasound mapping of serum anti-Müllerian hormone (AMH) levels, it emphasizes that AMH should not be used as an independent diagnostic test.
This review further examines the advanced methodologies driving modern PMOS research, including genome-wide association studies (GWAS), which investigate risk alleles across diverse human ancestry, and advanced microfluidic platforms (e.g., the “LATTICE” organ-on-a-chip framework) that allow researchers to study three-dimensional cellular interactions and accelerate automated high-throughput drug testing under PMOS-like hormone levels.
Review the findings
In this review, studies using automated AMH assays revealed that diagnostically, serum AMH levels >3.2 ng/mL in women aged 23 to 35 years may serve as a surrogate candidate for PCOM assessment, with a sensitivity of 88.6% and a specificity of 80.3%. In a diagnostic bioinformatics study, a machine learning model utilizing specific hormone values, specifically luteinizing hormone (LH), follicle-stimulating hormone (FSH), estradiol, and sex hormone binding globulin (SHBG), successfully predicted the onset of PMOS before clinical onset with an area under the curve (AUC) of up to 0.85 in out-of-sample testing.
The review also identified a strong genetic component, noting that 60% to 70% of daughters born to mothers with PMOS will develop the condition themselves. It also highlights how different reproductive and metabolic phenotypes may carry different risk profiles, reinforcing the need for more precise classification.
On the therapeutic front, a clinical update shows that the aromatase inhibitor Letrozole achieves significantly higher live birth rates for ovulation induction compared to the traditional option, clomiphene citrate (27.5% vs. 19.1%). Drug repurposing studies also highlighted that the antimalarial drug artemether attenuates hyperandrogenism, irregular estrous cycles, PCOM, and subfertility in PCOS-like rodent models by targeting ovarian enzymes and inhibiting excessive androgen synthesis. In a small human pilot study, the related compound dihydroartemisinin was associated with decreased hyperandrogenism, lower AMH levels, decreased PCOM, and normalized menstrual cycles.
conclusion
This review highlights that PMOS is a multifaceted and highly inherited disease that requires individualized and precise care rather than a one-size-fits-all approach. Although current treatments primarily manage symptoms such as abnormal bleeding and metabolic dysfunction with combined hormonal contraceptives (CHCs), lifestyle interventions, and metformin, the results of this review indicate that the future of PMOS treatment may depend on identifying common biological pathways and clinically meaningful subtypes.
Encouragingly, new treatments such as neurokinin 3 (NK3) receptor antagonists and glucagon-like peptide 1 (GLP-1) receptor agonists and multi-agonists have shown early or context-specific clinical potential in alleviating hyperandrogenism and improving metabolic and reproductive function, although some approaches remain preclinical and GLP-1 therapy requires caution with regard to conception and pregnancy. Addressing current diagnostic gaps and validating distinct reproductive metabolic subphenotypes through machine learning will enable future clinicians to intervene earlier, which could change the long-term health trajectory of millions of women.
Click here to download your PDF copy.
Reference magazines:
- JL Chan, I Masini, MD Pisarska (2026). Polyendocrine-metabolic ovarian syndrome (PMOS)/polycystic ovarian syndrome (PCOS): current and future trends. Journal of Clinical Research, 136(12). Doi: 10.1172/JCI202824. https://www.jci.org/articles/view/202824