

From gait speed and DNA methylation to AI scans and clinical texts, a major review maps how scientists measure aging and why the field needs stronger evidence before these tools can guide patient care.
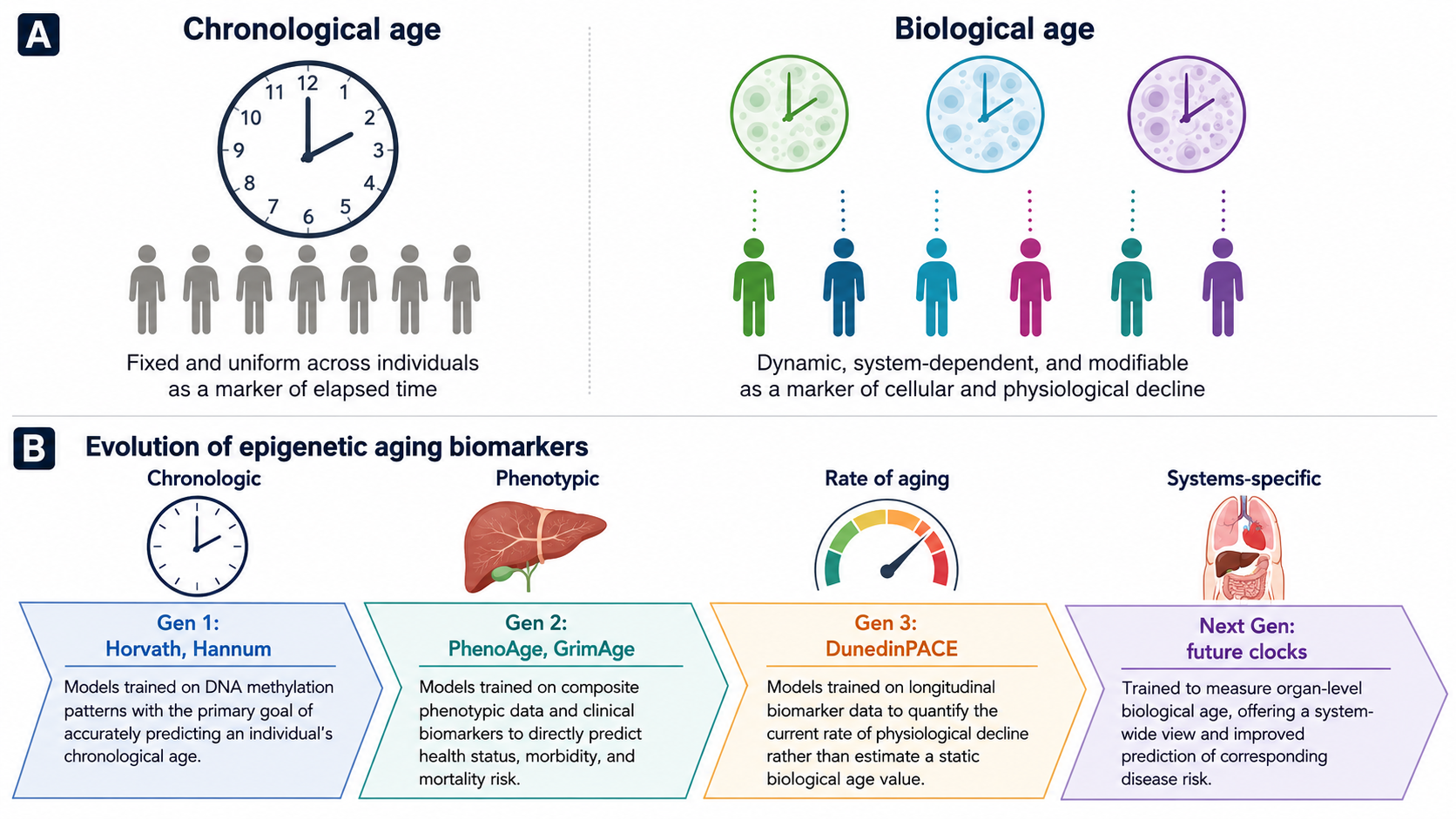
Distinction between CA and BA and progression of the epigenetic clock over multiple generations. (a) Chronological age reflects a fixed time scale, whereas biological age reflects cellular and physiological decline. (B) First generation clocks (Horvath, Hannum, etc.) were trained to predict chronological age. Second generation clocks (PhenoAge, GrimAge, etc.) focus on phenotypic health and mortality risk. Third generation clocks (such as DunedinPACE) measure the current rate of biological aging. The next generation of clocks aims to measure organ-specific biological age. Image adapted from Figure 1 of Cheema, BS et al. Functional, molecular, and digital measurements of biological age. Clinical Research Journal. 2026;136(12):e205777. doi:10.1172/JCI205777. Licensed under CC BY 4.0.
In a recent review published in clinical research journalIn , researchers discuss advances in biological age (BA) estimation over the years and ongoing limitations that need to be addressed for future clinical applications.
Until prospective validation, clinicians may ultimately use these approaches to identify high-risk individuals and support more individualized prevention or treatment strategies, but their role in daily practice remains unresolved.
People of the same sex born in the same year and with similar clinical profiles such as obesity may differ in physical performance, immune resilience, likelihood of developing disease, and overall survival. It reflects the cumulative effects of aging shaped by environmental exposures, health behaviors, genetic predispositions, molecular changes, and chance events. Biological age (BA) can capture such individual-level variation.
Scientists are developing new strategies to determine the biological age of various cells, tissues, and organs. Such efforts may support precision medicine approaches and ultimately improve standard of care.
In this review, researchers provide an overview of BA estimation approaches and ongoing challenges and limitations.
Traditional and modern methods for biological age estimation
Early age estimation models primarily used predefined variables, risk factors, and functional markers (such as gait speed and grip strength), and the results were interpreted as delayed or accelerated aging. They also developed a composite score for physiological aging. Although these methods can help estimate disease risk, they typically cannot account for differences at the cellular level that can affect mobility, strength, and balance, which can affect the ability to perform daily tasks.
Researchers are currently integrating molecular profiling and artificial intelligence (AI) algorithms into an integrated framework to improve BA estimation. While first-generation clocks such as Horvath and Hannum used supervised machine learning models based on selected CpG methylation sites to estimate chronological age, later clocks were designed to better capture phenotypic aging, morbidity, and mortality risk.
Digital AI models can analyze images, electrophysiology, wearable signals, and clinical texts, while large-scale language model (LLM)-based approaches have shown promise in estimating phenotypic aging from regularly collected health examination reports and electronic health records.
Decreased walking speed and grip strength are associated with decreased physical function and increased risk of death. New models use video-derived and computer-based analysis to make these assessments more scalable.
As people age, the lining of their arteries becomes less efficient. Flow-mediated dilation provides an ultrasound-based window into endothelial function, and pulse wave velocity and pulse pressure capture relevant aspects of atherosclerosis and vascular aging.
Wearables and digital monitors may contribute continuous data on heart rate, activity, sleep, and associated physiological patterns, while ECG-derived measurements such as age, inflammatory biomarkers, and maximal oxygen uptake provide a complementary window into cardiovascular and systemic physiological reserves.
Elevated levels of natriuretic peptides such as NT-proBNP can help estimate long-term cardiovascular disease risk at levels well below standard measurements. Similarly, the renal marker cystatin C outperformed traditional creatinine-based indicators in predicting mortality risk.
Deep learning models can estimate BA from brain magnetic resonance imaging (MRI) scans and high-resolution retinal vascular images. Advanced ML models can also use facial image processing to predict survival outcomes for cancer patients. Molecular profiling can also capture age-related biological patterns, potentially improving risk stratification. For example, elevated PAI-1 levels in middle-aged women are associated with a worsening metabolic and cardiovascular profile.
BA estimation using combined approaches such as the Klemera-Doubal method and PhenoAge, and DNA methylation clocks such as GrimAge and DunedinPACE have improved the determination of mortality risk by combining clinical biomarkers, biological processes, and methylation-based aging signals.
New clocks such as Systems Age, OMICmAge, GlycanAge, and MileAge can quantify changes across multiple organ systems, immune cell populations, and metabolic pathways. Proteomic aging clocks (PACs) use regression models to analyze thousands of proteins and can help estimate BA, health span, disease susceptibility, and mortality risk.
Challenges and future direction
The scientific community has made great strides in age estimation. Still, some challenges remain. There is no standardized uniform framework for determining an appropriate BA measure. Furthermore, most BA models rely on cross-sectional analysis and prognostic information.
Understanding whether changes in BA measurements reflect actual improvements or declines in health status requires direct comparisons of methodological reliability, response to treatment, feasibility, and long-term stability.
Scientists also need to improve AI models to address information transparency and depict age-related changes from disease pathophysiology for biomedical applications. Because predictive associations do not prove modifiable causality, researchers must also determine whether lower BA estimates correspond to meaningful improvements in health span, function, or survival. Coordinating multidisciplinary efforts and increasing investment in health services to link BA measures and clinical outcomes can help close these gaps.
To accelerate the clinical application of BA measures, prospective studies involving human participants and unified testing measures are needed.
conclusion
Based on this finding, advanced biological age estimation methods generally show strong predictive potential compared to traditional approaches. The new framework uses AI and machine learning to analyze multimodal data such as medical records, laboratory values, clinical findings, imaging results, and genetic information.
Although these integrated frameworks have the potential to capture complementary aspects of aging beyond traditional single-modality approaches, direct comparative and longitudinal evidence remains limited. However, further research is needed to link BA estimates and clinical findings and apply them to real-world settings.
Click here to download your PDF copy.
Reference magazines:
- Cheema, B. et al. (2026). Functional, molecular, and digital measurements of biological age, The Journal of Clinical Investigation, 136(12):e205777. Doi: 10.1172/JCI205777, https://www.jci.org/articles/view/205777