

A 50-year study has found that the global spread of Ebola is far more limited than public fears suggest, and that source control, infection prevention, and rapid response remain the strongest defenses.
Rapid communication: The risk of global spread of Ebola virus is low: Epidemiology of Ebola cases outside Africa from 1976 to May 2026. Image credit: Peterschreiber.media / Shutterstock
In a recent study published in the journal euro monitoringResearchers have reassessed the global threat of Ebola virus infection. This study analyzed historical data from 1976 to May 2026 to understand whether the recent outbreak of Bundibugyo virus disease caused by Bundibugyo virus, the ortho-Ebola virus that causes Ebola hemorrhagic fever, in the Democratic Republic of Congo in May 2026 should be considered a cause for global concern.
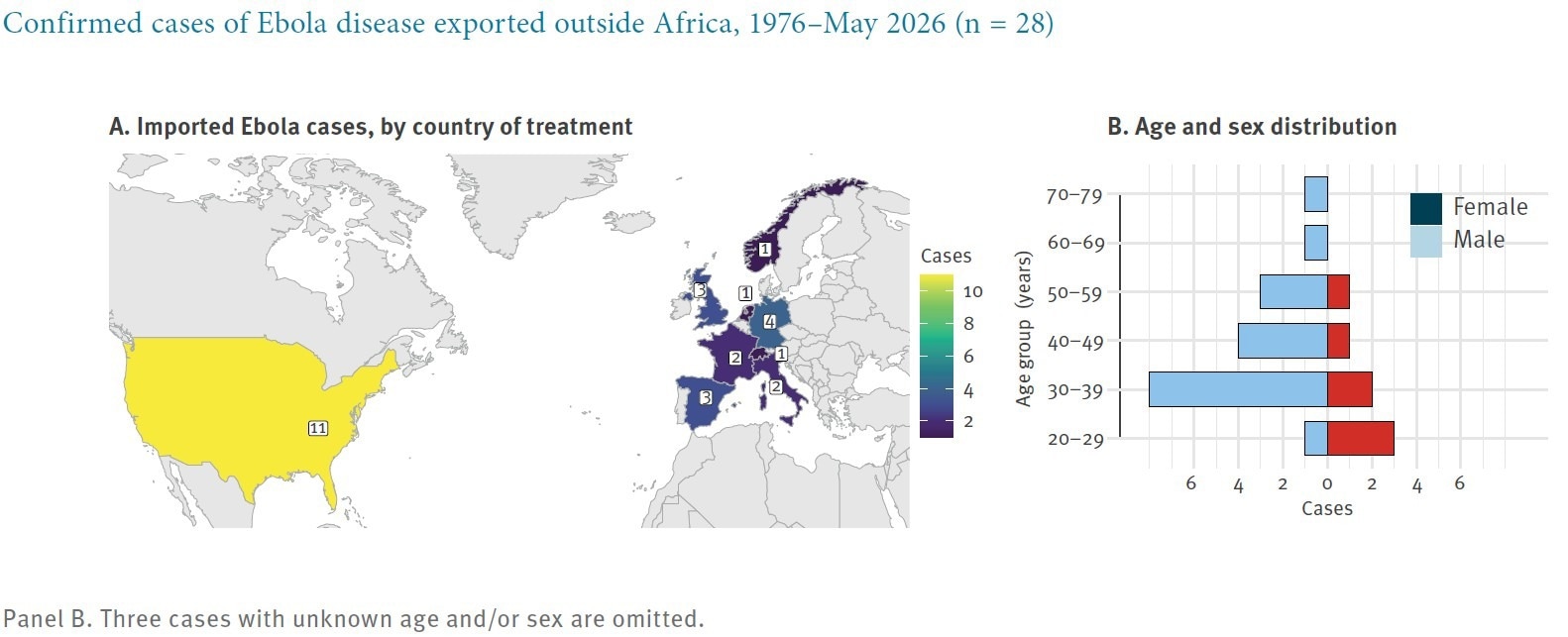
The study results showed that of the thousands of cases in Africa over 50 years, only 28 occurred outside the continent, indicating that international spread is rare and the risk of undetected transmission outside Africa remains extremely low.
background
In May 2026, an outbreak of Bundibugyo virus disease was reported in the Democratic Republic of the Congo, and additional cases were subsequently detected in Uganda.
Public health agencies issued border and travel guidance in response to the outbreak, a message that quickly reignited global fears over the recent coronavirus pandemic and the devastating 2014-2016 Ebola outbreak in West Africa.
Reviews in this field highlight that, historically, public fear during viral outbreaks often outweighs actual epidemiological data. Although the Ebola virus is highly lethal, its transmission dynamics differ from efficient respiratory infections such as COVID-19 and influenza, as human-to-human transmission generally requires direct contact with infected body fluids.
Nevertheless, scientists remain wary because the dense international aviation network could serve as a theoretical infection vector allowing naturally restricted pathogens to spread around the world.
About research
This study aims to distinguish international concerns and travel-related policy responses from historical evidence by drawing on decades of data to estimate an empirical threshold for Ebola to successfully breach continental borders. The study consists of an epidemiological review of historical data spanning from the first discovery of the virus in 1976 to May 2026.
Study data was collated through manual and artificial intelligence-powered searches of scientific articles, public health bulletins, news reports, and other sources, and results were matched against existing Ebola case lists. Past outbreak totals were extracted from sources such as the U.S. Centers for Disease Control and Prevention, the Humanitarian Data Exchange, and other public health records. This study specifically tracked all epidemic-associated infections identified outside Africa and categorized the identified primary export cases into two types: 1. Individuals who were intentionally evacuated for specialized treatment under strict biological containment, and 2. Travelers who crossed the border with a latent infection and developed symptoms during or after their trip. The authors also identified individual secondary infections acquired outside Africa while treating known Ebola patients.
The primary objective of this review was to determine the crude overall risk of international importation compared to the total number of African cases reported. The research analysis included rough risk calculations for outbreaks since 2000, and these data were considered most relevant to modern travel volumes and surveillance systems.
Research results
The study results revealed that over the entire 50 years of included data, only 28 confirmed cases associated with Ebola outbreaks could be identified outside Africa. Analysis of these cases further demonstrated that actual naturally occurring infestations are even rarer than they appear.
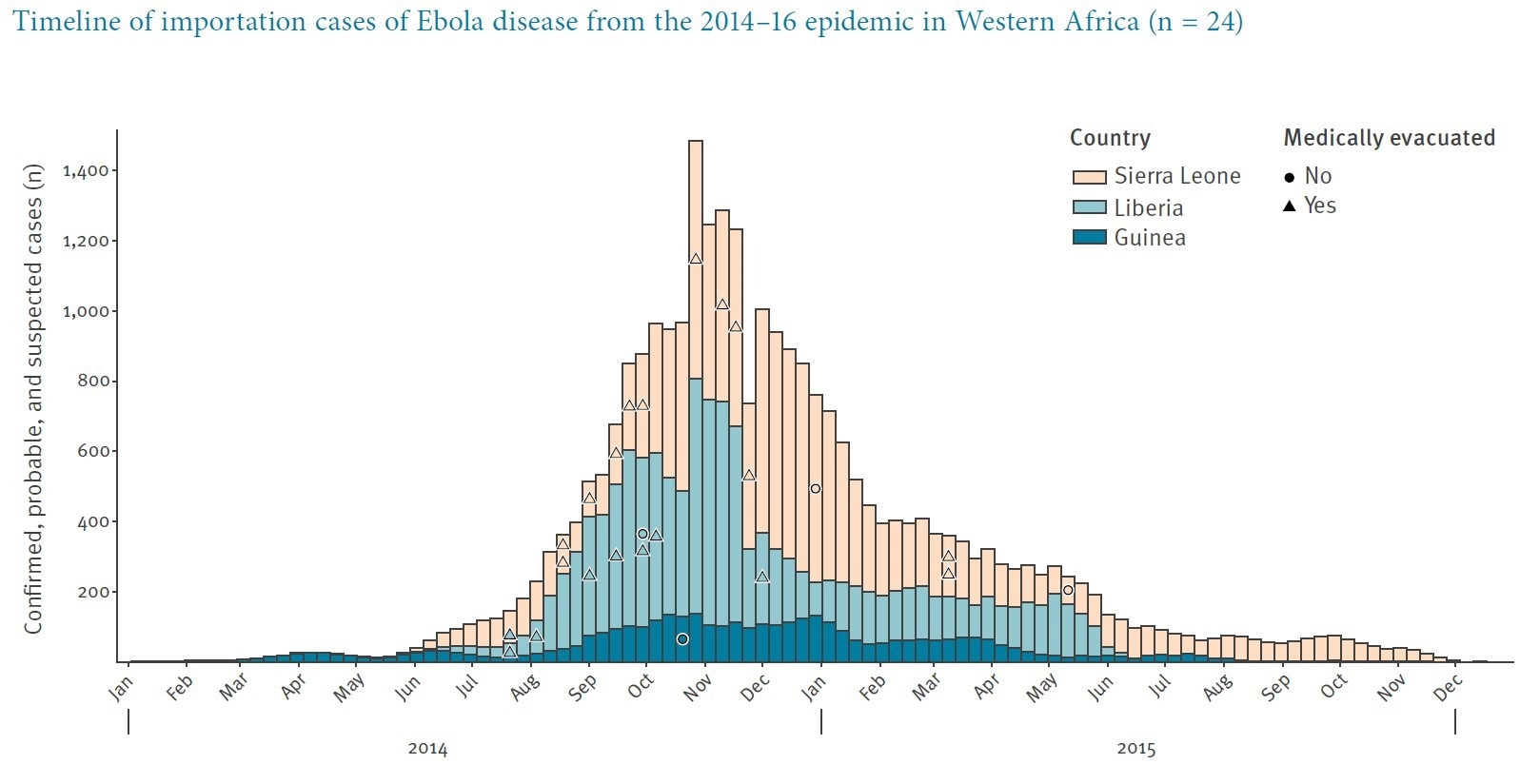
The majority of the 28 identified cases have been traced to people known to have been exposed occupationally or during the outbreak response, including healthcare workers, United Nations staff, and journalists. Most medical evacuations involved medical and response personnel being transported according to pre-arranged arrangements. Of the 28 cases, only four involved travelers who crossed the border during the incubation period and were diagnosed after passing the initial border check. All four potential cases occurred during the 2014-2016 Ebola outbreak in West Africa.
Focusing only on data since 2000, the study estimated that potential exports and their secondary cases accounted for 0.17 Ebola cases outside Africa for every 1,000 cases reported in the source outbreak. The crude risk for all exported cases, including medical evacuations, latent cases, and secondary cases, was 0.81 cases per 1,000 source cases. As a result, the authors concluded that the probability of an undetected latent infection reaching outside Africa has historically been very low, but noted that screening alone cannot detect asymptomatic individuals.
The study also found that 27 of the 28 exported cases occurred during the 2014-2016 West African Ebola outbreak, and one case so far has been linked to the 2026 Bundibugyo outbreak. There are no confirmed cases in Latin America and the Caribbean, Asia, or Oceania. During the 2014-2016 outbreak, the export risk per reported source case decreased by 4.6% per week and by 73% after the epidemic peak. This likely reflects increased infection prevention and control as response efforts scale up.
conclusion
The study shows that the threat of an uncontrolled global Ebola pandemic remains extremely low. Potentially deadly global health emergencies such as the Ebola outbreak require extreme vigilance, but current results from a thorough review of historical data suggest that intercontinental spread is rare and primarily involves people with known occupational or outbreak response exposures.
Despite these encouraging findings, the authors emphasize that the remarkably low estimated intercontinental transmission rates of potential export cases and their secondary cases should not be seen as an excuse for complacency.
They emphasize that the statistical safety described in the manuscript is dependent on sustained outbreak response, infection prevention and control, travel monitoring, and local public health capacity in affected areas. The authors also noted limitations such as possible lack of confirmation from non-English public health bulletins and geographically biased web-based searches.
The study concluded that the most effective means of preventing the spread of Ebola and similar pathogens outside their natural range is to control outbreaks directly at the source, particularly through local community-based case management and infection prevention and control measures.
Click here to download your PDF copy.